
Case Report | DOI: https://doi.org/10.31579/2692-9392/029
1 Department of Pediatric Pathology, Phoenix Children’s Hospital, Phoenix, AZ
2 Department of Pediatric Gastroenterology, Phoenix Children’s Hospital, Phoenix, AZ
*Corresponding Author: Shipra Garg, Department of Pediatric Pathology Phoenix Children’s Hospital 1919 East Thomas Road
Citation: Narry Savage, Emmanuel Siaw, Ashish Patel, Shipra Garg (2021) Ménétrier Disease; 2-Year-Old Boy Presenting With Prolonged Emesis, Generalized Edema and Chance Histopathological Finding of Cytomegalovirus Gastritis: A Case Report. J. Archives of Medical Case Reports and Case Study. 4(2); DOI:10.31579/2692-9392/029
Copyright: © 2021 Shipra Garg, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 February 2021 | Accepted: 02 April 2021 | Published: 12 April 2021
Keywords: ménétrier disease; emesis; hypoproteinemia; cytomegalovirus; hypertrophic gastropathy
Ménétrier disease (MD) is characterized by enlarged gastric folds with associated protein losing gastropathy. In children it is a rare and self-limited cause of protein losing gastropathy. We report a case of a 2-year-old male who presented with prolonged, refractory emesis and peripheral edema. Workup revealed severe hypoalbuminemia, hypoproteinemia, iron deficiency anemia, and high stool alpha-1 antitrypsin. Hepatic protein synthesis was normal with no urinary protein loss. Endoscopy showed antrum sparing, severe erosive gastritis in body and fundus, characteristic of MD. Histologic examination displayed inflammation with eosinophilia, foveolar hyperplasia, atrophic oxyntic epithelium, and rare CMV inclusions. Patient received antiviral therapy, intravenous albumin, diuretic and was discharged on high protein diet. Follow-up revealed clinical recovery, with endoscopy and histology showing normal gastric mucosa throughout the stomach. It is important to remain vigilant of this condition in pediatric population and to include it in the differential diagnosis in cases of protein losing gastroenteropathy.
MD is a rare disease typically found in adults, beginning insidiously with epigastric pain, nausea, vomiting, and generalized edema, it gradually becomes increasingly symptomatic with marked protein losing gastropathy [1] MD is considered a premalignant condition in adults being associated with gastric adenocarcinoma, often requiring gastrectomy. [2] In children, MD is rare, presents with identical symptomatology as in adults, but has a starkly different clinical course, as it is a benign, self-limited condition, with mean duration of 5 weeks. [3]
We present a case of a child with protein losing gastropathy associated with chance finding of cytomegalovirus (CMV) inclusions in the gastric body mucosa. This case illustrates the importance of including MD in the differential diagnosis, even in the pediatric population. To date we report the second youngest patient afflicted with this disease reported in literature, the youngest being 5 months younger from South Korea. [4]
A previously healthy 27-month-old boy presented with three-week history of vomiting and lower extremity swelling. He was initially treated by his primary care physician with seven-day course of amoxicillin and ondansetron as needed for vomiting secondary to presumed streptococcal pharyngitis. His symptoms continued despite therapy, and peripheral edema was noted.
Past medical history included full term birth via vaginal delivery to a mother of advanced maternal age. He had regular prenatal and postnatal care, and regularly attended recommended well-child checks. He was fully vaccinated with no known allergies, and no surgical history.
Physical exam revealed an alert, tired, non-ill appearing toddler with generalized edema, most pronounced in bilateral lower extremities. His abdomen was mildly distended, without hepatosplenomegaly or masses. The remainder of the exam was unremarkable. Initial work up revealed marked leukocytosis with lymphocytic predominance, microcytic anemia, marked hypoproteinemia, and marked hypoalbuminemia. Liver function tests were within normal limits indicating normal hepatic synthetic function, and erythrocyte sedimentation rate and C-reactive protein did not indicate active inflammation. Urinalysis was negative for protein, eliminating a renal etiology for hypoproteinemia. Pro-brain natriuretic peptide was within normal limits, ruling out cardiac etiology for edema. Serum quantitative PCR for CMV was positive, with Helicobacter pylori, Epstein-Barr virus, and celiac studies all negative. High level of stool alpha-1 antitrypsin was present.
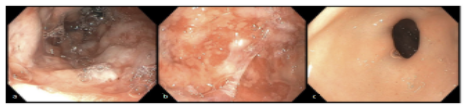
Upper endoscopy revealed severe erosive gastritis involving gastric fundus and body, with normal mucosa in the gastric antrum (Figure 1).
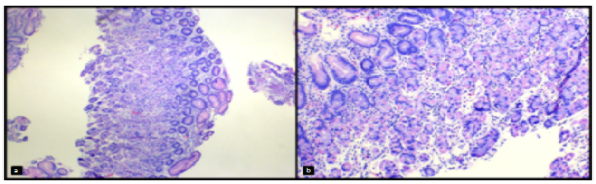
Histological evaluation of gastric biopsies of the fundus body revealed mucosal erosion, active inflammation with eosinophilia, edema of the lamina propria, foveolar hyperplasia, cystic dilatation of pits, and atrophy of oxyntic epithelium. Cytomegalovirus inclusions were identified within epithelial cells, verified with immunohistochemical staining (Figures 2a, 2b and 2c). No Helicobacter pylori organisms were seen. No abnormalities were seen histologically in the gastric antrum.

Histological findings of foveolar hyperplasia, oxyntic epithelial atrophy, and CMV inclusions in conjunction with endoscopy findings of gastritis with hypertrophic gastric folds, and clinical findings of peripheral edema, hypoproteinemia, hypoalbuminemia, elevated levels of stool alpha-1 antitrypsin, and positive CMV serology were all consistent with the diagnosis of Ménétrier disease.
Valganciclovir and a proton pump inhibitor therapy were initiated for erosive gastritis, along with albumin infusions and furosemide. Patient was discharged on a high protein diet, and continued antiviral, ferrous sulphate and PPI therapy. On his follow-up visit 4 weeks later, he experienced complete resolution of symptoms. Follow-up gastric endoscopy and histology at 3 months showed normal mucosa throughout, with mild remnant foveolar hyperplasia in gastric body (Figure 3).
Pediatric MD is an uncommon, acute, self-limited hyperplastic gastropathy characterized by foveolar hyperplasia and oxyntic epithelial atrophy resulting in protein losing gastropathy [5]. Patients typically present with non-specific symptoms including epigastric pain, nausea, emesis, diarrhea, anorexia, and peripheral edema, sometimes with a history of a viral prodrome. Laboratory studies will reveal hypoalbuminemia, hypochlorhydria, and elevated stool alpha-1-antitrypsin level.
Initial imaging with ultrasound can detect hypertrophic rugae, [6] with endoscopic evaluation revealing the enlarged gastric folds of fundus /body and unremarkable antrum. It may be associated with several infectious agents such as CMV, adenovirus, enterovirus, Helicobacter pylori, mycoplasma, herpes virus, and giardia lamblia, [7] with one case documented to be caused by Clostridium difficile. [8]
CMV mediates the changes in the gastric epithelium via increased expression of transforming growth factor alpha (TGF-α), causing mucus cell proliferation resulting in foveolar hyperplasia. Widened gap junctions between the overabundant foveolar cells permit increased protein leakage from the vasculature into the gastric lumen which is excreted in the stool. [3] This mechanism of protein loss due to CMV is further supported temporally; the resolution of symptoms of hypoproteinemia coincides with the eradication of the infection.
Treatment of Ménétrier disease is directed towards the causative microorganism for gastritis, if one has been identified. Otherwise treatment is symptomatic and supportive in nature. Intravenous albumin can be administered followed by a diuretic such as furosemide to reduce edema and the patient is advised to maintain a high protein, low fat diet. Mean duration of illness is approximately 4-6 weeks.
Besides MD, other clinical conditions that can give rise to protein-losing gastropathy with hypoalbuminemia and subsequent edema include; cardiac failure, malnutrition, impaired hepatic synthesis, excessive renal loss, intestinal lymphangiectasia, or intestinal mucosal inflammation with dysregulated protein permeability.
Diseases showing thickened gastric folds can mimic MD at endoscopy. These conditions range from foveolar hyperplasia in reactive conditions to malignancy. Hypertrophic lymphocytic gastritis shows prominent intraepithelial lymphocytes. Other rare conditions differentiated via histology include Zollinger-Ellison syndrome (characterized by normal foveolar epithelium with parietal cell hyperplasia and hypertrophic hypersecretory gastropathy (hyperplasia of all glandular components) which may or may not be associated with protein loss. Crohn’s disease characteristically has gastric granulomas on histology. Peutz-Jeghers syndrome and hyperplastic polyps show foveolar hyperplasia with architectural distortion. Gastric lymphoma and carcinoma are exceedingly rare in children, will display effacement of the mucosa by infiltrating malignant cells Thus endoscopy with histologic correlation should be performed on all suspected cases of gastric mucosal hyperplasia to adequately narrow the differential diagnosis.
In conclusion, our case emphasizes the need to include pediatric Ménétrier disease in the differential diagnosis for a young child with an abrupt onset of vomiting and gastrointestinal protein loss. This case further supports a causal relationship between CMV infection and pediatric Ménétrier disease, highlighting the importance of including this organism as a possible causal agent for this condition.
Conflict of interest: None funding source: None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
